|
|
Ossification of the Posterior Longitudinal Ligament
OPLL
General Considerations
- Heterotopic ossification of the posterior longitudinal ligament
- Occurs primarily in cervical, most often C4-C5, next most commonly in thoracic spine and least frequently in lumbar spine
- Most commonly in 40s and 50s
- Twice as common in males as females
- Higher prevalence in Asian population, especially Japanese
- Since OPLL can narrow the spinal canal, most who are symptomatic present with spinal stenosis or myelopathy
- Associated with DISH
Clinical Findings
- Majority of patients have no symptoms
- Cervical myelopathy is the most common presentation
- Numbness
- Neck pain
- Weakness
Imaging Findings
- Linear ossification immediately posterior to vertebral body in canal
- May be continuous (spans several bodies and intervening disc spaces), segmental (occupies back of body but spares disc spaces) or both
- Predominantly in high cervical spine
- CT is best at demonstrating ossification
- On MR, signal behind the vertebral bodies and interbody spaces becomes less dense on all MR imaging sequences as disease progresses
Differential Diagnosis
- Calcified herniated disc
- Calcified meningioma
- Calcified epidural hematoma
Treatment
- Symptomatic patients may undergo decompression such as by laminectomy
Prognosis
- Patients with mild cases of OPLL on first discovery rarely progress to severe stenosis
- Patients presenting with myelopathy are likely to progress


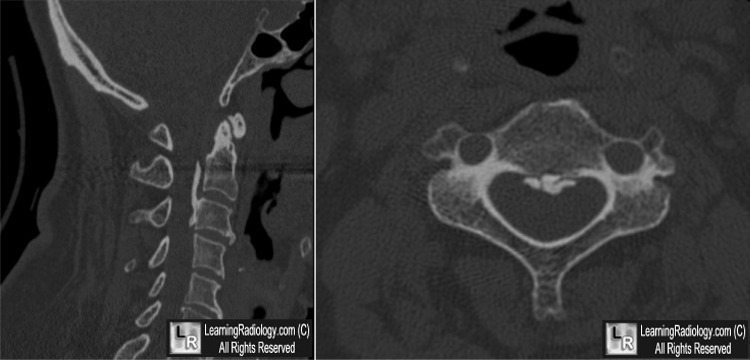
Ossification of the Posterior Longitudinal Ligament (OPLL). Above:Linear ossification just posterior to the posterior border of the cervical vertebral bodies (white arrows). Below: Sagittal reconstruction of cervical spine CT on left shows same flowing ossification (yellow arrow); axial CT demonstrates the ossified posterior longitudinal ligament (blue arrow).
For these same photos, click here and here
For more information, click on the link if you see this icon 
Inamasu J et al: Ossification of the posterior longitudinal ligament: an update on its biology, epidemiology, and natural history. Neurosurgery. 58(6):1027-39; discussion 1027-39, 2006
|
|
|

{kind=link}
{kind=link}